Filter by


As part of BAU Accreditation Readiness activity, a NSQHS Standard of the Month program has been introduced. This involves a focus on one Standard per month, with communications and walkarounds to help staff be aware of how Best Care at Western Health reflects this Standard, to ask staff possible Surveyor questions and answers, and to walk in a Surveyor’s shoes to see what WH practice looks like.
We are excited that NSQHS Standard 7: Blood Management is to be the focus of the second Standard of the month. This will run from Tuesday 2 April to Friday 26 April. Look out for friendly Fab 5 team members, Best Care Co-ordinators, and other staff who will visit clinical areas/departments to discuss Blood Management with you.
During the month, we will also have a specific focus (with prizes) on all things blood.
Our ‘Fab 5’ team includes blood management CNCs, nursing, medical, education, and quality expertise to support our ongoing compliance with NSQHS Standard 7 – Blood Management.
The good news is we are already providing Best Care and living up to the requirements of NSQHS Std 7 in our everyday work! It is why we performed so well at the December 2023 Accreditation Survey.
Please continue reading to find out more about our Blood Management strategies, achievements and opportunities for improvement, as well as resources to help you to continue to be Accreditation Ready for NSQHS Standard 7.
Michelle Read
NSQHS Std 7 ‘Fab 5’ Team Lead
Director of Nursing & Midwifery
The NSQHS Standard 7 – Blood Management Standard aims to ensure patients’ own blood is safely and appropriately managed, and that any blood and blood products that patients receive are safe and appropriate.
Programs and strategies to help support Blood Management at Western Health include:
- Informed patient consent for blood and blood products
- Use of key performance indicators, incident and adverse reaction reporting, and audits to review and enhance blood and blood product management
- Blood and blood product policies, procedures and protocols which support clinical practice in line with National Patient Blood Management Guidelines
- Participation in the Victorian State Haemovigilance Reporting Scheme.
- Blood product and transfusion medicine educational resources for clinical and ancillary staff
- Optimisation and conservation of patient’s own blood
- Equipment and processes to minimise blood and blood product wastage
The following resources have been put together to support staff to be aware of the NSQHS Blood Management Standard and Accreditation Ready for Survey against this Standard:
- NSQHS Standard 7 Accreditation Walkaround Questions and Answers
- Spotlight on Blood Management – Know Your Standard
- Health Standards (NSQHS) WeLearn Module
{kind=link}

“Our family live in regional Victoria and have two young boys. Over the past decade, we have seen and benefited from the generosity of so many Australians through life-saving blood donation. Throughout this time, we have received large amounts of blood products, in a range of healthcare settings in both regional and metropolitan Victoria.
Over the years, I have had several health concerns which have required multiple transfusions of red blood cells, plasma and platelets. These transfusions have saved my life.
I also suffered significant blood loss during the birth of our two boys, as both were born extremely premature. During the course of my pregnancies, I had several antenatal bleeds which required anti-D injections to prevent haemolytic disease of the newborn which could have been life-threatening to my boys.
When our oldest boy was born at 27 weeks, he required multiple blood transfusions during his stay in the Neonatal intensive care unit (NICU). Following his admission, he continued to have ongoing health concerns as a result of his premature birth.
Our second boy was born at the beginning of the COVID-19 pandemic at just 23 weeks, and like his older brother, he has had significant health issues due to his premature birth. Over his life, he has received in excess of 40 blood transfusions, over 15 transfusions of platelets and plasma, as well as multiple iron transfusions.
Since the birth of our two boys, our family has spent several extended periods of time separated from one another. During this time, many of our family and friends would ask us what they could do to help. Generally, we would politely decline, but then we thought of something they could do – not just for our family but for so many others like us – they could give blood.
My husband and I decided to create a team so our friends and family could support our boys and the countless other recipients in need. Many of our team members have expressed how thankful they are for us encouraging them to get back into donating or starting to donate. We even had family and friends send us photos during their donation, letting us know they were doing this for our boys. Seeing and hearing these things each time a team member donates, brings us so much joy. Knowing that their selfless actions and generosity are literally saving lives, and making a difference to so many people and their families, fills us with gratitude.
For a while, being home together as a family of four, didn’t look like it was going to be a reality for us, but with the help of countless individuals, including generous blood donors, it is the reality we are now living. There are no words to express just how grateful we are to each and every person who has ever donated. Regardless of how many or how few donations a person has been able to make, these donations have changed and saved lives.”
There are multiple improvement initiatives underway to improve Blood Management. Do you know about these?
- Mandatory training on We learn.
- Blood Champion portfolio initiative
- Patient experience and understanding of consent surveys
- Transfusion alert cards & information pamphlets
- Subcutaneous Immunoglobulin business case
- Advanced scope of practice course for applicable nursing staff
- New Massive Transfusion Protocol audit in collaboration with the Anaesthetics Department
- Use of Multi-Unit Transporters and shippers for blood products to prevent blood wastage
- Communication boards in patient facing spaces across all sites
- Managing Blood Transfusion reactions – procedure for clinical staff.
- Correct patient identification checks.
We are proud of …
- Completion of Blood Safety mandatory training increasing across the health service.
- Embedding Blood safety training into all induction programs for medical and nursing staff at Western Health
- The successful amalgamation of all blood processes across Western Health:
- Including the development of multiple new policies to ensure safe and compliant practices
- Removal of all blood products from pharmacy monitored refrigerators, and into blood validated blood refrigerators
- Introduction of a new blood product (Fibrinogen Concentrate) including onsite storage for emergency critical bleeding cases
- Transference of audit results onto the Performance Dashboard – a central platform accessible to all Unit Managers
- Re-introduction of the Blood Management Newsletters following a halt over the Covid-19 pandemic
- Introduction of the Transfusion Alert Cards and information pamphlets for patients with specific transfusion requirements
- Successful roll out of the use of Group O+ red blood cells for patients in meeting a specific criteria, in alignment with the National Blood Authority’s recommendations
- Establishing safe processes for changes of patient ID details in the context of the massive transfusion protocol.
We are looking forward to …
- Transitioning to the New Footscray Hospital in 2025
- Establishing meaningful improvements following the Patient experience and understanding of consent to blood transfusions
- The update of the WeLearn Blood management module – with an anticipated increase in clinician completion rates
- Development and introduction of a Cell Saver Policy, Procedure and Guideline
- Reviewing and improvement blood information sheets provided to patients – including information in different languages
Our focus continues on …
- Providing safe and timely care to patients around all things blood
- Updates around the Massive Transfusion Protocol are appropriate, effective and safe – as MTPs remain a high-risk clinical scenario for the use of blood products
- Ensuring clinicians are well informed on all blood processes, and are aware of the policies and procedures around safe administration
- Identification of high blood users, monitoring of key risk areas and providing targeted education and support for these specialty areas
- Why use 2, when 1 will do campaign
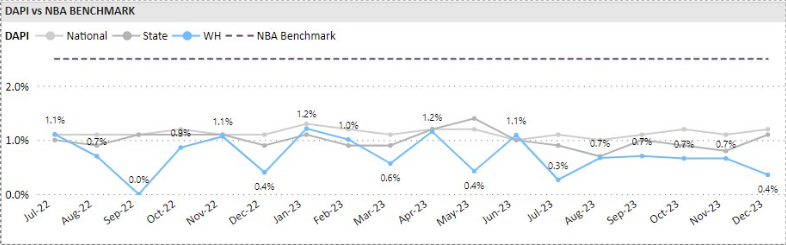
Wastage of Blood Products
Red blood cells which are prescribed for patients who have clinically significant anaemia – this can be for various underlying reasons. Red blood cells are the most frequently transfused blood product at Western Health.
Donated red blood cell units have a life span of 42 days after which time they cannot be given to patients and must be discarded. For red blood cells that have been manipulated (for example – irradiated), this lifespan shortens.
For this reason, we work very closely with our pathology service providers to continually review the stock (inventory) of blood products keep onsite and rotate our stock as necessary to prevent blood wastage.
We measure our performance against the State and National discard percentages provided by Lifeblood monthly.
Western Health’s red cell unit discard rate is consistently lower than the State and National discard percentages.
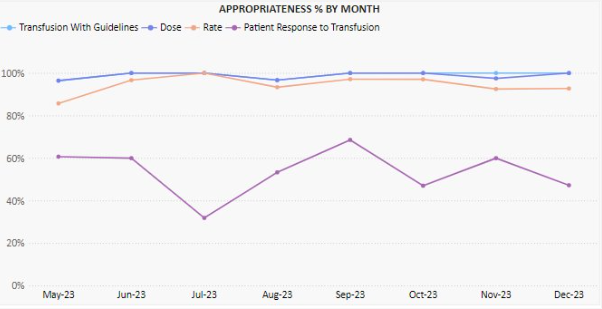
Appropriate Use of Blood Products
Australia has one of the safest blood supplies in the world, however the transfusion of blood products is not without risk and can lead to complications and adverse outcomes for patients. Blood transfusions should only be given if the potential clinical benefits outweigh the potential risks to the patient.
As part of our Blood Management clinical audit program we undertake regular audits of transfusion episodes to review Western Health’s alignment of practice against the National Patient Blood Management Guidelines
Of the two hundred and ninety-nine red cell transfusion episodes audited between May 2023 and December 2023, 99.1% were assessed as being aligned with the National Patient Blood Management Guidelines.
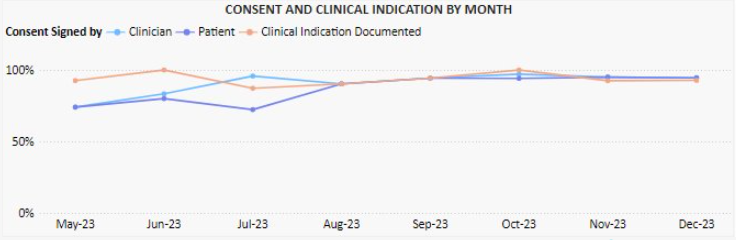
Documentation of Blood Product Administration
One of the NSQHS Standard 7 criterion ensures that the documentation relating to all blood products can be traced from vein (donor) to vein (recipient).
As part of our Blood Management clinical audit program, we undertake regular audits of transfusion episodes to review Western Health’s alignment of practice against the National Patient Blood Management Guidelines
These audits are performed monthly, and monitor:
- Documentation of informed consent
- Documentation of transfusion details (i.e., batch number, start/stop times and date, authorised checkers etc)
- Documentation of cold chain (for remote blood refrigerators)
Of the two hundred and ninety-nine red cell transfusion episodes audited between May 2023 and December 2023, 83.3% had clinical indication for transfusion documented. Over the same time period, documented signing of consent to transfusion by both clinicians and patients has significantly improved.

The Clinical Communiqué is an electronic publication containing narrative case reports about lessons learned from Coroners’ investigations into preventable deaths in acute hospital and community settings. The Clinical Communiqué is written by clinicians, for clinicians.
Associate Professor Nicola Cunningham
Welcome to the first issue of the Clinical Communiqué for 2024. In this edition we are looking at the challenging aspects of determining fitness to drive in older drivers. Advancing age is associated with co-morbidities that cumulatively increase driving risk and will affect a person’s fitness to drive. Stroke, dementia, sleep disorders, mobility issues, hearing and vision impairment may warrant cessation of driving. The two cases in
this edition demonstrate two main risk profiles in older drivers – the driving risks when a patient is bodily capable but easily disorientated, and the driving risks when a patient is mentally sharp but physically slow. A diagnosis of dementia or a physical impairment does not automatically signify a patient should lose their licence, but it does herald the need for notification to the licensing authority and an assessment of fitness to drive.
This is not the first time The Communiqués team have shared important learnings from coronial cases about fitness to drive. We explored the theme in a previous edition of the Clinical Communiqué (September 2015 Edition Volume 2; Issue 3) where we featured three case summaries and an expert commentary from Australia’s leading forensic medical experts in traffic medicine. The edition highlighted the complexities surrounding driving ability in patients with a range of chronic medical conditions, and the role of their treating practitioners. In those cases, hypoglycaemia, seizures, and visual impairment were each found to be contributing factors in fatal collisions. Associate Professor Morris
Odell’s expert commentary on the complexities of considering fitness to drive in the context of the effect of the condition on the ability to perform the tasks of driving, and the jurisdictional differences in reporting, is as important and relevant today as it was then.
Although the focus this time is on older drivers and how to ensure driving safety in the setting of age-related cognitive and physical changes, the fundamental messages are the same:
1. A person’s suitability to hold a licence is a question that should be asked early in a therapeutic relationship.
2. It is crucial to perform a comprehensive driving assessment with input from multidisciplinary sources about a person’s medical conditions – their abilities and limitations, and their driving history.
3. Legal obligations and licensing guidelines should be understood by all health professionals. As Dr Gaya cogently wrote in the previous fitness to drive edition, “Driving is not a right, but a privilege…subtle effects of a fairly common medical condition in a driver can disastrously
impact on the driver and other road users. For this reason, it is incumbent on both drivers and their healthcare professionals to further extend their therapeutic relationship to consider the impact of their conditions and treatments on driving.”
As well as the importance of understanding the steps involved in assessing driving ability in a patient, health professionals must also appreciate the key impacts of a loss of licence for a patient. It represents a loss of independence, with reduced mobility, confidence and autonomy, potentially leading to social isolation and depression. In employed patients this can also have a negative economic impact.
Dr Angela Sungaila returns in this latest edition with a case summary, and the expert commentary is by another leading expert in the field of fitness to drive, Professor Dimity Pond who is a general practitioner, researcher, and educator with a special interest in dementia.
Professor Pond’s commentary shares insights about fitness to drive in older drivers from the perspective of the patient, the health professional, and the system. Her gentle and proactive approach to the issue is one that we should all adopt for our patients. Don’t avoid the conversations and do explore what assistance and limitations might need to be put in place. Driving is an activity that benefits every one of us, so we all play a role in keeping road users safe.
Click on the image to access the March 2024 Clinical Communique


 As part of BAU Accreditation Readiness activity, a NSQHS Standard of the Month program has been introduced. This involves a focus on one Standard per month, with communications and walkarounds to help staff be aware of how Best Care at Western Health reflects this Standard, to ask staff possible Surveyor questions and answers, and to walk in a Surveyor’s shoes to see what WH practice looks like.
As part of BAU Accreditation Readiness activity, a NSQHS Standard of the Month program has been introduced. This involves a focus on one Standard per month, with communications and walkarounds to help staff be aware of how Best Care at Western Health reflects this Standard, to ask staff possible Surveyor questions and answers, and to walk in a Surveyor’s shoes to see what WH practice looks like.
We are excited that NSQHS Standard 6: Communicating for Safety is to be the focus of the first Standard of the month. This will run from Monday 4 March to Friday 29 March. Look out for friendly Best Care Co-ordinators, Fab 5 team members, and other staff who will visit clinical areas/departments to discuss Communicating for Safety with you.
During the month, we will also have a specific focus on the use of Communication Boards and staff engagement in the new Clinical Handover training module.
The Communicating for Safety Standard aims to ensure there is effective communication between patients, carers and families, multi-disciplinary teams and clinicians, and across the health service organisation, to support continuous, co-ordinated and safe care for patients.
The good news is we are already providing Best Care and living up to the requirements of this Standard in our everyday work! It is why we performed so well in the December 2023 Accreditation Survey.
Please continue reading to find out more about our Communicating for Safety strategies, achievements and opportunities for improvement, as well as resources to help you to continue to be Accreditation Ready for NSQHS Standard 6.
Douglas Mill
NSQHS Std 6 ‘Fab 5’ Team Lead
Director of Nursing & Midwifery
The NSQHS Standard 6 – Communicating for Safety is aimed at improving communication within healthcare organisations and reducing the risk of harm to patients.
Western Health’s comprehensive approach to Communicating for Safety draws upon the requirements of this Standard and supports the monitoring, review and improvement of safe care. Programs and strategies to help support communicating for safety include:
- Communication learning packages to support staff knowledge and use of effective communication techniques.
- Reviewing clinical incidents to look for themes around clinical communication and identify areas for improvement.
- Clinical handover protocols to support good communication between our healthcare teams and clear documentation of patient information.
- The use of an electronic medical record to help ensure patient information is easily accessible and up-to-date, which can improve communication between the healthcare team.
- Key roles and responsibilities related to patient identification processes across clinical and clerical workflows.
The following resources have been put together to support staff to be aware of the NSQHS Comprehensive Care standard and Accreditation Ready for Survey against this Standard:
The following resources have been put together to support staff to be aware of the NSQHS Comprehensive Care standard and Accreditation Ready for Survey against this Standard:
- NSQHS Standard 6 Accreditation Walkaround Questions and Answers
- NSQHS Standards at a Glance
- Health Standards (NSQHS) WeLearn Module
Using ISBAR
After an unexpected death in one of our chronic care services, the family were obviously distressed. Being a very spiritual family the operations manager used the ISBAR process to communicate the need for urgent pastoral care.
The pastoral care manager was able to quickly understand the situation and what was required and had pastoral care support on site with the family within 30 mins.
The family were very grateful for the support in this difficult time.
Using the information provided, the manager recognised that other patients may have been traumatised in the unit and facilitated a pastoral care visit for each of the other 20 patients.
Without the use of ISBAR the urgency of this situation would have been delayed. There is no doubt that it allows fast and accurate transfer of information to ensure our patients and carers receive best care.
There are multiple improvement initiatives underway to improve Communicating for Safety. Do you know about these?
- WeLearn package to set the standard for Clinical Handover has been rewritten to make it contemporary and applicable to all craft groups
- Reviewing clinical incidents to see look for themes around clinical communication to identify areas for improvement continues at every meeting of the committee
- Replacement of the electronic program to allow the discharge record to go straight to the GP
- Clarifying key roles and responsibilities related to patient identification processes across clinical and clerical workflows.
- Monitoring the use of appropriate electronic communication platforms
- Release of the new communication boards to all wards
We are proud of…
- Refocusing on use of ISOBAR/ ISBAR in handover processes through an updated Clinical Handover PPG and accompanying WeLearn module extended to all staff
- Use of EMR data as part of dashboards to inform patient care in timely manner (e.g. overdue cannulae)
- The extensive and active involvement of Language Services across Western Health to ensure patients and their carers and families are kept informed about clinical care and treatment planning
- EMR 2.1 GoLive in July which brings clinical services into the one EMR to increase visibility of the patient journey and to reduce fragmentation of information (reducing hybrid workflows)
- Updating ‘What Goes Where’ staff resources as we transition from current systems to the EMR to help staff navigate to the relevant source of information to ensure they have the full picture
- Re-establishing routine audits (eg Consent, Handover) to inform improvement approaches
- Updating and standardizing patient communication boards across WH
- Supporting staff to publish ward round information on EMR in a more timely and effective manner.
We are looking forward to…
- Further developing KHWD boards in clinical areas to share achievements, areas of improvement with patients/ relatives and staff.
- The introduction of the replacement interface to allow discharge summaries to be sent directly to GPs.
Our focus continues on…
- Developing Clinical Handover PPG and Welearn packages to support the exchange of clinical information.
- Re-establishing audits (Patient ID, Consent, Time-Out) to inform improvement approaches.
- Reviewing Riskman data to identify themes of communication incidents to strengthen WH clinical communication capability.
- Continuing to uplift discharge summary sharing with GPs and external health services/ sharing of clinical information between WH and BM&M sites which supports continuity of care.
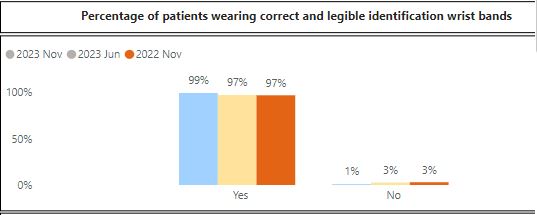
Patient Identification
Patient identification is crucial for providing safe and effective healthcare. It ensures that each individual receives the right care, medications, and treatments, while minimising the risk of errors.
Patient wrist bands play a key role in correct identification and procedure matching.
Results from the November 2023 Advancing Best Care (ABC) Audit showed that 99% of patients on audit day were wearing correct and legible identification wrist bands.
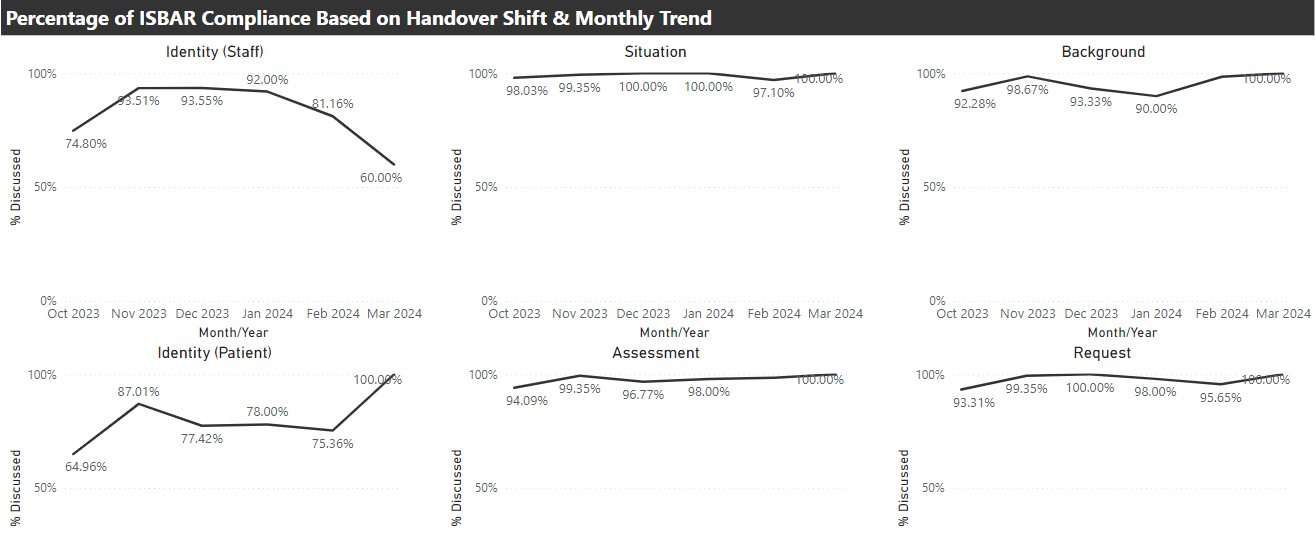
Clinical Handover
Clinical handovers are vital for patient safety. They enable clinicians to exchange critical information about a patient’s condition, treatment, and needs when there is a change of staff shift or transitioning care. Effective handovers ensure continuity and prevent mistakes.
The ISBAR tool is a valuable asset in clinical handovers. It stands for Identify, Situation, Background, Assessment and Request. Western Health uses ISBAR to help clinicians communicate efficiently and ensures crucial information is passed accurately. It’s a simple but effective way to support best care. Following expansion of the use of our Electronic Medical Record (EMR), more staff and services are supported to consistently apply the principles of ISBAR to clinical handovers.
Clinical handover auditing shows good use of ISBAR.
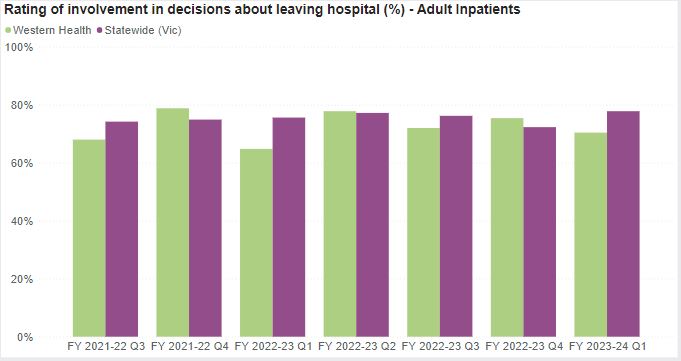
Discharge Planning
Discharge planning and communications are essential for best care. They help ensure a smooth transition from the hospital to home or another care setting. By coordinating post-hospital care and medications, it enhances patient recovery, reduces readmissions, and promotes overall well-being. In essence, discharge planning is a key part of comprehensive and effective healthcare.
The Victorian Health Experience Survey (VHES) includes patient feedback on planning for discharge from our inpatient services. The Department of Health and Human Services has a target of 75% of very positive responses to questions on discharge care.
The following graph shows the percentage of our patients who provided very positive responses to questions on discharge planning, care and communication to end September 2023. Our results tend to fluctuate between being above and below the Statewide average
Western Health continues to upload patient information to the My Health Record to the Australian My Health Record, a secure and centralised online system storing important health information for consumers. The Australian Digital Health Agency has launched its first consumer mobile application (’My Health’), which enables users to more easily access My Health Record information.
At a local level, Western Health continues to explore better ways of sharing health care information with the General Practitioners (GPs) of consumers using our health care services.

![]() This edition we would like to acknowledge the FHED and Access teams who received a Best Care award for Coordinated Care in relation to Footscray Short Stay Unit Flow.
This edition we would like to acknowledge the FHED and Access teams who received a Best Care award for Coordinated Care in relation to Footscray Short Stay Unit Flow.
The Short Stay Unit is crucial in achieving the flow required to see new patients in a timely manner. The team identified two interventions to implement in the unit – capping the number of patients admitted to the SSU and allowing better flow by defining criteria for direct admission. By implementing these changes the unit was able to see measurable improvement in the way the SSU ran but also the whole of the ED.


A 72 year old female was admitted to Ward 2C on the 15th September 2023. She had been recently discharged from hospital to a new RACF but represented within 38 hours due to ongoing behavioral issues secondary to a history of Alzheimer’s Disease and Vascular Dementia with Behavioural and Psychological Symptoms of Dementia.
On arrival to the ward, the patient was identified as a high Occupational Violence and Aggression risk and required multiple code greys to manage her behaviours of concerns. Although she had an Additional Care Resource to support her care, her behaviours were challenging for the multidisciplinary team to manage.
A behavioural management plan was developed and included medication reconciliation, planned code greys, use of Greek music and dolls as a distraction. Her family were also involved in the planning of her care. The outcome was positive with better management of her behaviours of concerns.
The patient was transferred to the treating teams home ward several days later, where she became unsettled and had an altercation with another inpatient. She was transferred back to 2C, where her behaviours quickly settled again. This story demonstrates the quality of care provided by the 2C team and highlights their ability to develop relationships and manage difficult behaviours well.
A transfer to the Dementia Management Unit was planned for the patient while work continued on her discharge planning.
Well done to all staff involved in the care of this patient with a complex condition and needs.

“My father was recently admitted to 3E, I understand there was a serious incident, and my father was transferred to Cath lab for the duration of his stay.
There was an in-charge on Saturday morning, who actually did a double shift (not sure her name) and in her hectic day she went above and beyond her job description by keeping me updated regarding my fathers’ management.
I also have to commend an ANUM from 3E who on Sunday took some time and went searching for my father’s missing belongings while coordinating his discharge. She was reassuring in her delivery of care to me.
While we always hear the negative, I want to acknowledge the above as well as all the staff on the ward who took great care and showed compassion to my elderly father. They managed to keep it all together in a frightening situation.
I am proud to say I work for Western Health and how we work not only as a team but a family.
I feel that this needs to be highlighted for all to see.” (From a WH staff member)
There are multiple improvement initiatives underway across EMA. Do you know about these? (If not, feel free to ask your manager).
• Standardised Operating Processes for the Bed Coordinator teams to improve time to allocate beds from ED• Implementation of Virtual communications between our Urgent Care Centres and main Emergency Departments, improving clinical support to Urgent Care
• Ongoing access and flow initiatives across our EDs, including the use of Short Stay Units, AV Offload, Front of House and Fast-Track models, Category 2 time to be seen, use of Lower West Ward at Williamstown
• Comprehensive Care Improvement project across our EDs and Urgent Care Centres, focusing on nursing leadership and risk assessment and tools, including FirstNet implementation/utilisation and revision of audit tools and processes
• Timely Emergency Care Collaborative (TECC) aiming to improve the timeliness of emergency care through improving system-wide patient flow – PDSA cycles continue within the ED & inpatient stream: Timely Emergency Care Collaborative – Home (sharepoint.com)
We are proud of…
• Maintaining timely access to care for all of our patients – AV offload within 40 minutes was 75% at FHED in November!
• Ongoing recognition of our staff achievements across the Division
• Paediatric Emergency in-situ and interdisciplinary simulation program
We are looking forward to…
• Reviewing our Sunshine Behavioural Assessment Unit, Hub and Fast-Track models of care with key stakeholders to ensure they are providing Best Care for our patients
• Establishing our new Emergency Medicine Intranet site
• Establishing an ED/HiTH collaboration project
• Sunshine ED refurbishment
• Review of General Internal Medicine model
• EMR implementation at Bacchus Marsh and Melton
• Improving patient access to our EMA outpatient clinics through the use of guidelines and other improvement initiatives
Our focus continues on…
• Addressing our Falls & Pressure Injuries across the Division
• Improved compliance with risk assessments and utilisation of iPOCS across our inpatient areas
• Improving medical and nurse practitioner staffing (particularly across our EDs and Urgent Care Centres)
|
Data Analysis |
Key Message |
||||
|
Hand Hygiene |
Period 2 of National Hand Hygiene Initiative (NHHI) ended in October with a Divisional result of 89.1% (target = 80%). | Don’t forget to replace the end of bed alcohol-based hand rub if empty. If you do not know where to get a new bottle from in the ward or department, please let the nurse in charge know. | |||
|
Medication Errors |
|
Don’t forget the 5 Rights for medication safety |
|||
|
Comprehensive Care—Falls, Pressure Injuries and nutrition |
|
|
|||
|
Mechanical Restraint |
There have been fewer episodes of Mechanical Restraints across the Division in November and we continue to see improved compliance with appropriate care and documentation.
|
Use least restrictive practice, review and remove as soon as possible. Ensure it is documented. |
|||
| Communicating for Safety | There were 10 incidents related to the Communicating for Safety Standard, with six of these being in our Emergency Departments and Urgent Care Centres. | Please visit our Best Care website for more information about Standard 6 | |||
| Blood Management | There were two blood management incidents across our Division in November – one on 2C and one in FHED. | Complete your mandatory training via WeLearn | |||
| Recognising and responding to Acute Deterioration | There were five reported clinical incidents related to Standard 8 in November, four of which were in our EDs and Urgent Care Centres |
See more about Standard 8: Deteriorating Patient |
| Incidents and Complaints |
|
Standard 1 and Standard 2 |
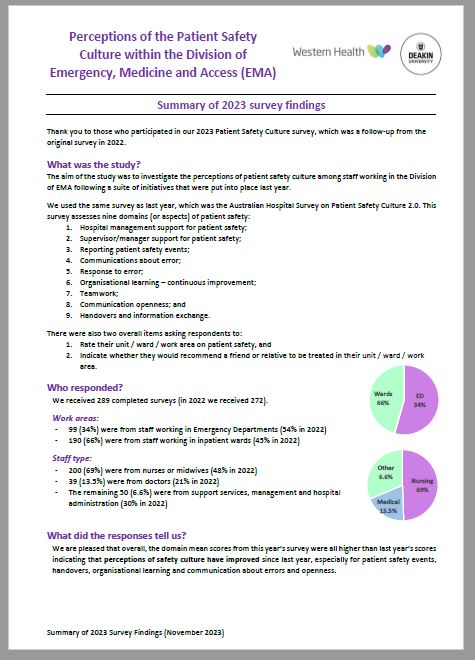
Click on the image to view the Summary of 2023 Survey Findings


Welcome to the December edition of VAHI news. We’ve got a lot to share this month, as work we’ve been doing over the year is coming to fruition on some key projects. VAHI has been working with partners across the health system to progress initiatives that are going to improve health outcomes for Victorians, now and in the future.
We’ve hit a major milestone in our partnership with Victoria’s six Primary Health Networks (PHNs), with an agreement in place that allows two-way data sharing between the department and PHNs. The agreement will help PHNs understanding how Victorians use services in geographic areas, which will assist in service planning and delivery. In early December, the department and all six Victorian PHNs will meet to discuss other opportunities for data sharing to support joint projects. There’s shared optimism that increased visibility of the data will translate into real action that improves peoples’ care.
VAHI is supporting GenV, a statewide research program that aims to create a picture of the health and wellbeing of an entire generation of Victorians using linked data. VAHI’s Centre for Victorian Data Linkage is partnering with the project to link data from more than 115,000 Victorian children and parents creating a linked data asset that will be used for years to come. And while we’re on the Centre for Victorian Data Linkage, we also update you on improvements to their secure platform for data analytics, VALT2.
A partnership between VAHI and Eastern Health is set to improve the collection, collation and use of consumer feedback, and the experience and care for patients across our health system. The collaboration is looking to create an environment where consumers are empowered to share their experiences in a way that feels right for them. Eastern Health have recently come on board to lead consultations with health services, and their expertise will guide how the sector is engaged in this important work.
I am pleased to advise that our Hospital Acquired Complication (HACs) dashboard was re-launched last week and is again available to authorised users of the VAHI portal. The dashboard supports health services to identify and understand variation in the level of complications their patients experience. The updated dashboard enables services to investigate their HACs and use the learnings to design improvement activities.
Finally this month, as we head towards the end of the year, I would like to thank you for your support, and wish you a happy and safe holiday season. We look forward to working with you in 2024.
Don’t forget to subscribe to VAHI news if you haven’t already, and encourage your colleagues to do the same. It’s the best way to keep up to date with all the latest from VAHI. Likewise, if you’ve got a story to share about how VAHI data has helped you, we’d love to hear it. Contact VAHI Communications via vahi@vahi.vic.gov.au.
Sincerely,
Dr Lance Emerson, CEO
Using linked data to enrich Australia’s largest birth and parent longitudinal cohort – GenV

GenV (short for Generation Victoria) is a statewide research program that aims to create a picture of the health and wellbeing of an entire generation of Victorians using linked data. VAHI’s Centre for Victorian Data Linkage (CVDL) is partnering with the project to link data from more than 115,000 Victorian children and parents creating a linked data asset that will be used for years to come.
VAHI and Eastern Health join forces to improve the collection and use of consumer feedback

The Victorian Agency for Health Information (VAHI) is partnering with Eastern Health as the first phase of a broader project to improve the collection, collation and use of consumer feedback. Eastern Health have recently come on board to lead consultations with health services, and their expertise will guide how the sector is engaged in this important work.
Data sharing agreement set to improve service planning and innovation

The Victorian Department of Health has recently developed an umbrella information sharing agreement with each of Victoria’s six Primary Health Networks (PHNs). The agreement has patient privacy and security of information at its foundation, while allowing for two-way data sharing between the department and PHNs.
HACs dashboard returns with risk-adjustment to aid statewide view

A major update of VAHI’s Hospital-acquired complications (HACs) dashboard was released on the VAHI Portal last week.
The dashboard supports health services to identify and understand variation in the level of complications their patients experience.
Access to linked data easier than ever with VALT2

The Centre for Victorian Data Linkage has implemented an updated version of its secure data access environment, the Victorian data Access Linkage Trust. VALT2 enables dissemination of linked data within a secure-based cloud environment, with analysis undertaken via Virtual Machines (VMs).
![]()
Our current primary focus for the Division is preparation for accreditation. As you will all be aware, Western Health is scheduled for a short notice accreditation visit (WH will be notified 2 business days before the accreditation begins), which is likely to occur in November. Please ensure you and your staff are familiar with our Best Care site and all information and resources related to accreditation. Our managers are completing weekly readiness checklists in order to assess gaps and ensure we are prepared.
One of our primary focus areas for Quality and Safety across the Division is Comprehensive Care and there are a number of initiatives underway including an Improvement Project in our EDs and Urgent Care Centres; improving our utilisation of the Comprehensive Care iPOC for inpatients; and ensuring all risk assessments and strategies are in place.
“I just wanted to take this opportunity to give positive feedback on my recent visit to the Emergency Department at Western Hospital. I have a chronic condition, atrial fibrillation, that I am aware can be a bit of a pain for EDs as it’s usually non-life threatening yet can be quite unpleasant for the person experiencing it (albeit that at least some of that may be the result of anxiety associated with the condition) and does carry risks in the long term.
My condition has unexpectedly worsened recently, and I have found it hard to find the balance between avoiding burdening a busy ED, and being responsible about my health by getting timely help when things seem serious (due to the severity or duration of the AF episode). I have had two recent attendances at Western ED and really appreciated the attitude and care of the health care team. I felt like the dilemma I experienced was acknowledged and respected. Interestingly knowing that I would be taken seriously (after the first presentation), made the second presentation a far calmer and more orderly experience. I suspect this helped me to contain my symptoms. I await an operative procedure that I hope will be successful. However, in the meantime we arrived at a plan to avoid further ED attendances and to define more clearly when they might be needed.
I felt like this was something we worked out collaboratively and respectfully in the interests of both myself and the appropriate future use of the ED”.
Well done to the Footscray Hospital Emergency Department nursing team on their recent pulse check for Nurse Pool and Nurse Bank. The pulse check is coordinated through the Nursing and Midwifery workforce unit to gauge how pool and bank staff feel supported and valued in various wards and departments. The FHED team scored above organisational averages in the area of team work, staff satisfaction and meaningful work. Thank you FHED nursing team for making pool and bank nurses feel part of your team to provide best care to our patients.
You may have noticed the EMA leadership team in your areas undertaking leadership walk arounds. Leadership walk arounds are not new to EMA. The walk arounds provide us with an opportunity to connect with our teams, observe best care in action and also hear and act on your feedback. A recent systematic review published in BMJ Open Quality assessed the impact of leadership walkarounds on operational, cultural and clinical outcomes. The authors concluded that evidence exists to suggest a positive association of leadership walk-arounds on operational and cultural outcomes. The article can be found at: Impact of leadership walkarounds on operational, cultural and clinical outcomes: a systematic review | BMJ Open Quality
There are multiple improvement initiatives underway across EMA. Do you know about these? (If not, feel free to ask your manager).
Standardised Operating Processes for the Bed Coordinator teams to improve time to allocate beds from ED.
General Internal Medicine Ward Round Standardisation project.
Thunderstorm Asthma Preparation.
Code Crimson and Sepsis alert development in our EDs.
Ongoing access and flow initiatives across our EDs, including the use of Short Stay Units, AV offload, Front of Hours models, Category 2 time to be seen, use of Lower West Ward.
Improvements in utilisation of Transit Lounge.
Comprehensive Care Improvement project across our EDs and Urgent Care Centres, focusing on nursing leadership and risk assessment and tools.
Timely Emergency Care Collaborative (TECC) aiming to improve the timeliness of emergency care through improving system-wide patient flow – PDSA cycles continue within the ED & inpatient stream: Timely Emergency Care Collaborative – Home (sharepoint.com)
We are proud of…
• Maintaining timely access to care for all of our patients.
• Our Footscray ED and Access team won a Best Care Awards for improved utilisation of SSU.
• Our Williamstown ED received a Bank Vic $5K innovation grant to purchase laptop on wheels.
• Dr Maninder Mundae (WH Rheumatology) was successful in a WH Shark Tank grant for Ultrasound Clinic.
• Our Medical Diagnostics Unit was Nominated for an Inspire Award.
• We have been managing our complaints well across the Division.
We are looking forward to…
- Accreditation readiness
- Mental Health and Wellbeing Act implementation & compliance and improving the use of our Sunshine BAU and Hub.
- SHED refurbishment.
- Review of General Internal Medicine model.
- EMR implementation at Bacchus Marsh and Melton.
- Improving patient access to our EMR outpatient clinics through the use of guidelines and other improvement initiatives.
- Setting up a PDSA cycle with the ICU team to improve daily flow from ICU.
Our focus continues on…
- Addressing our OVA incidents across the Division.
- Falls & Pressure Injuries remain a key focus across the division.
- Improved compliance with risk assessments and utilisation of iPOCS across our inpatient areas.
- Completion of the required mandatory training and performance development plans for all our staff.
- Improving medical and nurse practitioner staffing (particularly across our EDs and Urgent Care Centres).
|
Data Analysis |
Key Message |
||||
|
Hand Hygiene |
Overall Hand Hygiene compliance for the Division was 89% in October 2023, which is similar to last month. | Don’t forget to replace the end of bed alcohol-based hand rub if empty. If you do not know where to get a new bottle from in the ward or department, please let the nurse in charge know. | |||
|
Medication Errors |
|
Don’t forget the 5 Rights for medication safety |
|||
|
Comprehensive Care—Falls, Pressure Injuries and nutrition |
|
|
|||
|
Mechanical Restraint |
There has been an increase in the number of episodes of Mechanical Restraints in October, however we have seen improved compliance with appropriate care and documentation.
|
Use least restrictive practice, review and remove as soon as possible. Ensure it is documented. |
|||
| Communicating for Safety | There were 13 incidents related to the Communicating for Safety standard and the majority (8) of these were in our Emergency Departments and Urgent Care Centres. | Please visit our Best Care website for more information about Standard 6 | |||
| Blood Management | There was six blood managements incident across our Division in October- all of these were in our EDs/SSU. | Complete your mandatory training via WeLearn | |||
| Recognising and responding to Acute Deterioration | There were 9 reported clinical incidents related to standard 8 in October, 7 of which were in our EDs and Urgent Care Centres. |
See more about Standard 8: Deteriorating Patient |
| Incidents and Complaints |
|
Standard 1 and Standard 2 |

NSQHS ACCREDITATION BULLETIN OCTOBER | 2023
Welcome to the October 2023 NSQHS Accreditation Bulletin.
This publication has been developed to provide key messages and information about preparing for org-wide NSQHS Accreditation Survey.
For those who would like to just view a summary of this Bulletin, click on the four headings below:
- Key Messages October 2023
- Upcoming Milestones
- Resource Centre
- Contact for Accreditation Questions/Support
For those who would like a more comprehensive read, continue reading the Bulletin sections below or select areas of interest from the index to the right.
Best Care Governance & Support Division
We have developed a plan to activate when we are given our 24 hour notice that Accreditation Surveyors will be visiting Western Health. Note: We will be given notice on a Thursday, with a Survey commencing on the Monday and concluding on the Friday.
This plan includes a number of ways to notify staff, services and patients, including emails, PA announcements and screen savers.
Communication will tell staff to access the home page of the Live Best Care site. A big banner with a link to FAQs and tools with be visible to support you through the Accreditation Survey. The link will take you to the following page which will be updated when survey is announced: NSQHS Accreditation Survey FAQs and Tools – Live Best Care (wh.org.au)
The National Safety and Quality Health Service (NSQHS) Standards provide a nationally consistent statement of the level of care consumers can expect from health services. NSQHS Standards compliance activity and accreditation surveys supports us to monitor, review and continually improve Best Care.
The eight NSQHS Standards are:

- From 1 July 2023, no scheduled accreditation surveys; only short-notice assessments with 24 hours notice. We will be notified on a Thursday that a week long survey will commence on the Monday.
- As WH’s current NSQHS Accreditation status lapses in May 2024, the short-notice assessment will be at some point between 1 July 2023 and 31 December 2023. It is looking likely survey will happen fairly close to November 2023.
- We will have a team of approximately 13 accreditation surveyors visiting all of our campuses for a week
- Accreditation surveyors will return 65 days post survey if there are any recommendations from Survey
- Surveyors will spend up to 75% of survey time in clinical wards and departments providing or supporting care and facilities
- Transitioned Mental Health services will be included in survey
- Dame Phyllis Frost Centre will not be included in this survey

In order for ACHS to confirm the number of Surveyors required for Accreditation Survey and link us with a Lead Surveyor for Survey planning, a number of documents have been submitted to ACHS, These include a full listing of WH campuses, services, bed numbers/activity and workforce numbers. Transitioning mental health service details were included in the documentation as well as WH Clinical Trial activity which is a new focus for accreditation survey.
A NSQHS Standard short notice response plan was activated when we had mock accreditation survey in June. Thank you to staff who replied to our survey about how this went. Activation appeared to go smoothly, with positive feedback from staff.
A centralised NSQHS Standard evidence portal for Surveyors while on site at WH has been completed.
 NSQHS Standard Fab 5 Teams have gone from strength to strength, and are working in conjunction with key Western Health committees to ensure our Best Care quality systems are being used to continually monitor, review and improve organisation-wide compliance against the NSQHS Standard requirements. Each team has as a minimum designated nursing, medical, allied health, education and best care co-ordinator leads.
NSQHS Standard Fab 5 Teams have gone from strength to strength, and are working in conjunction with key Western Health committees to ensure our Best Care quality systems are being used to continually monitor, review and improve organisation-wide compliance against the NSQHS Standard requirements. Each team has as a minimum designated nursing, medical, allied health, education and best care co-ordinator leads.
Led by Nursing Leads (Directors of Nursing & Midwifery) and supported by BAU Action Plans, the Fab 5 Teams are having an impact. Each Team has completed what will become annual organisation-wide WH Practice Summaries and Reflective Compliance Reviews against their aligned NSQHS Standard and are driving/supporting clinical practice improvement.
Organisation-wide WH Practice Summaries have been updated to reflect current practice and highlight improvement activity against the NSQHS Standards. These documents will be added to the Live Best Care site.
The teams have also supported NSQHS ‘Standard of the Fortnight’ activity. Due to positive feedback on this initiative, it will continue in 2024, with a NSQHS ‘Standard of the month’ program implemented.
Current areas of focus for accreditation readiness:
- Excessive clutter – the hard rubbish collection at the start of October was a great success. ‘Embrace Your Space’ tips have also been distributed to support initiatives being planned to support areas decrease clutter
- Some areas have items such as dirty linen stored on the floor – ‘no more on the floor’ campaign launched
- Training and performance management to meet our targets – make sure you are up-to-date, with specific focus on lifting the rates of BLS and OVA training, as well as uploading PDPs to WH Register
- Clinical Auditing – a centralised clinical audit register has been developed, with links to surveys and results
- Shared development of patient goals and preferences – make sure you are using of the ‘About Me form’
- Improvements to medication storage and disposal – new medication disposal bins have been rolled out
- Screening and assessment processes to minimise patient harm across all sites – Bacchus Marsh Hospital going live with new risk assessment tools in the week commencing 24 October
- We need to be consistent in practice and use of WH (not localised) tools for handover – training materials on using the EMR to support clinical handover currently being distributed
- We need to be consistent in checking of points of patient ID for practices such as handover – WH PPG on points of patient ID revised
- KHWD Boards are a good tool, but there is opportunity to improve the way they are being used – guidelines & support for use of KHWD boards reviewed, with engagement start with front-line staff to update and fully understand their KHWD Board where indicated
As mentioned In last month’s Nursing & Midwifery News we are focusing on ensuring consistency of practice across our wards, areas, and departments to ensure we are all delivering Best Care safely and reliably.
The Managers Accreditation Checklist has been a useful tool in the past and has been reinvented with checklist items under the relevant NSQHS Standard; the Checklist is helpful in achieving the consistency in service delivery and best care that our consumers can expect across the organisation.
The Manager Accreditation Checklist has been incorporated in a Managers Accreditation Manual which contains the Checklist and Embrace your Space Tips.
The checklist contains items that require action to ensure the area and staff are prepared for NSQHS Accreditation; not all items on the checklist will be relevant to particular areas. Within the checklist some items may contain a hyperlink to an Embrace Your Space Tip.
The Embrace Your Space Tips are key messages for frontline staff with a practical solution for managers, assistant managers, and portfolio holders. The Embrace Your Space Tip provides practical information to action an item on the checklist.
Managers are responsible for completing the checklist and delegating items on the checklist as appropriate. The checklist should be completed monthly; managers are expected to re-visit the checklist for completion as needed and within 24 hours of receiving notice of NSQHS Accreditation.
This resource tool will be useful to remain prepared for short notice NSQHS Accreditation into the future.

Key initiatives included in the communications and engagement plan to support staff be ‘Accreditation Ready’ by end June 2023 have been reviewed for ongoing use.
The diagram to the left summarises activity that will continue as business as usual to maintain staff awareness and engagement in accreditation readiness.
The Live Best Care Microsite is our central information portal for staff on WH’s Quality Systems supporting Best Care and compliance with NSQHS Standards
The ‘Are you ready for NSQHS Accreditation?’ section of the Site contains FAQs and links to resources to help staff be ‘Accreditation Ready’
![]()
Our current primary focus for the Division is preparation for accreditation. As you will all be aware, Western Health is scheduled for a short notice accreditation visit (WH will be notified 2 business days before the accreditation begins), which could occur at any time. Please ensure you and your staff are familiar with our Best Care site and all information and resources related to accreditation. Our managers will be completing weekly readiness checklists in order to assess gaps and ensure we are prepared.
We continue to ensure improvement initiatives are ongoing in relation to ensuring timely access to care for our patients, as described in our Statement of Priorities. In September we have seen improvement in a number of these metrics compared to the month prior which means that patients are waiting less time for care in our community.
A 75yr old lady with multiple medical and legal complexities was admitted with bacterial epidural abscess and acute on chronic renal failure. Following a prolonged admission at Werribee and Footscray ICU, the patient was transferred to ward 2D for further management.
The patient advised the team that her listed Next Of Kin was claiming to be her Enduring Power Of Attorney against her wishes. The medical team sought legal advice and during her last weeks of life, the nursing team advocated for patient privacy and her wishes to not allow this person to visit. The multidisciplinary team worked collaboratively to ensure the patient’s long-time family friend was appointed Enduring Power Of Attorney, as per her wishes.
Prior to her deterioration, the patient instructed her friend to purchase thank-you gifts for all the staff (coffee, tea and chocolates) and made hand written thank you cards to individual staff who she felt provided very special care to her.
The patient unfortunately went into multiple organ failure and with the nursing team advocating for end-of-life care, the palliative care team was involved. This patient passed away with dignity and in comfort.
I took my daughter to Williamstown Hospital Emergency Department on 18/09/2023, she had cut her head open and required glue. Every single member of staff was so kind to her, the ladies on the front desk were extremely kind, the doctor and nurse were so wonderful. My daughter felt so comfortable and didn’t want to go home. Thank-you so much to all the team for working so hard and looking after everyone at the hospital. We are incredibly grateful for everything you do.
There are multiple improvement initiatives underway across EMA. Do you know about these? (If not, feel free to ask your manager).
Removal of handover sheets across all of our EMA wards
General Internal Medicine Ward Round Standardisation project
Thunderstorm Asthma Preparation
DOS, Access and ED huddle changes
Regular simulation sessions at Williamstown ED and our Urgent Care Centres (supported by our Sunshine Education and Simulation team)
2G Staff wellbeing project– focusing on self-care activities prior to a shift
Comprehensive Care Improvement project across our EDs and Urgent Care Centres, focusing on nursing leadership and risk assessment and tools.
Timely Emergency Care Collaborative (TECC) aiming to improve the timeliness of emergency care through improving system-wide patient flow – PDSA cycles continue within the ED & inpatient stream: Timely Emergency Care Collaborative – Home (sharepoint.com)
We are proud of…
- Opening our new GIM Ward 2H at Sunshine Hospital, which includes a transit lounge.
- 69 staff members within EMA to receive Length of Service Awards for 10-35 years of service (4 of these with 35 years of service).
- Improved rates of inpatient falls and hospital acquired pressure injuries.
- Improvements in timely access to care for our patients, including releasing ambulances to the community and our time to see patients in our EDs.
- Improved rates of Mandatory Training and Performance & Development Plan (PDP) completion.
We are looking forward to…
- Accreditation readiness
- Mental Health and Wellbeing Act implementation & compliance
- Sustaining and improving our timely access to care
- SHED refurbishment
- Review of General Internal Medicine model
- EMR implementation at Bacchus Marsh and Melton
- Endoscopy waitlist audit and access improvement initiatives.
Our focus continues on…
- Addressing our OVA incidents across the Division
- Falls & Pressure Injuries remain a key focus across the division
- Improved compliance with risk assessments and utilisation of iPOCS across our inpatient areas
- Weighing our patients – both on admission and weekly
- Completion of the required mandatory training for all our staff
- Improving medical and nurse practitioner staffing (particularly across our EDs and Urgent Care Centres)
- Improving waiting times for our patients requiring a Gastro-Intestinal Endoscopy procedure
|
Data Analysis |
Key Message |
||||
|
Hand Hygiene |
Overall Hand Hygiene compliance for the Division was 90% in September 2023, which is an improvement from last month. Some areas have yet to meet the audit numbers for the period. | Don’t forget to replace the end of bed alcohol-based hand rub if empty. If you do not know where to get a new bottle from in the ward or department, please let the nurse in charge know. | |||
| Healthcare Associated Infections | Nil. | Remove unnecessary cannulas as soon as possible. | |||
|
Medication Errors |
|
Don’t forget the 5 Rights for medication safety |
|||
|
Comprehensive Care—Falls, Pressure Injuries and nutrition |
Average weekly weight compliance across division is 84% and on admission is 66%. |
|
|||
|
Mechanical Restraint |
There has been a reduction in the number of episodes of Mechanical Restraints over the past two months, however compliance with appropriate documentation remains low.
|
Use least restrictive practice, review and remove as soon as possible. Ensure it is documented. |
|||
| Communicating for Safety | There were 20 incidents related to the Communicating for Safety standard and the majority (17) of these were in our Emergency Departments and Urgent Care Centres. | Please visit our Best Care website for more information about Standard 6 | |||
| Blood Management | There was one blood managements incident across our Division in September. | Complete your mandatory training via WeLearn | |||
| Recognising and responding to Acute Deterioration | There were 2 reported clinical incidents related to standard 8 in September, both in our EDs and Urgent Care Centres. |
See more about Standard 8: Deteriorating Patient |
| Incidents and Complaints |
|
Standard 1 and Standard 2 |